Living and dying well:
Reimagining palliative care
for older people
Living and dying well:
Reimagining palliative care
for older people
Briefing for policymakers
Policy context
By 2036, 2.6 million people in the UK are projected to be over 85 years old. This
age group will account for over 50% of all deaths. Older people living with frailty
and Multiple Long-Term Conditions (MLTC) will become the main recipients of
palliative care, yet there is limited evidence about their specific needs.1
There is inequity in access to palliative care in older age. Those without families are particularly vulnerable.2
There is a legal, moral and clinical imperative for palliative care services to support people with Frailty and MLTC as they near the end of their lives. Rethinking community care must include revisioning palliative care to support those living longer.3
Integrated Care Boards will be failing in their duty unless they listen to and understand the complex care needs of older people with progressive MLTC. Reconnecting Living and Dying requires upstreaming and aligning palliative care provision to local communities.4
Key research findings
Palliative care is often seen as focusing on the final stages of a terminal disease, determined by time until death. Older people, living and dying over time, face a double bind in accessing palliative care. Neither they, nor welfare services, view older people as appropriate for referral, and opportunities are missed to support living and dying as well as possible. Whilst older people may live with vulnerability, they are also resilient and capable, and this must be taken into consideration. Identifying the palliative care needs that matter most to older people with frailty/ MLTC requires the recognition of their strengths and concerns, as well as their physical needs, across a continuum of living and dying.
These include:
- Trust in care providers. Trust is eroded by high staff turnover.
- Not to feel lonely, alienated, and invisible.
- Opportunities to discuss current and future care needs.
- Support with administration and optimisation of medicines.
- Services and interventions to support mobility.
Supporting end of life provision for this growing and underserved population necessitates a shift to tailored multidimensional tools and community focused integrated care services.5 In other words: a person-centred approach.
Understanding frailty and multiple long-term conditions (MLTC)
Frailty is age-related and describes the gradual loss of inbuilt physiological reserves that leads to sudden, potentially fatal health deteriorations following seemingly small events, such as a minor infection.6 It is a longterm condition and closely linked with multimorbidity known as Multiple Long-Term Conditions (MLTC). MLTC refers to the presence of two or more long-term health conditions and is associated with increased mortality, lower quality of life, and greater use of healthcare services, including unplanned hospital admissions.
Older people living with frailty and/or MLTC who are coming towards the end of their lives may have many weeks, months or even years to live. There is a requirement for easy and consistent access to a variety of non-specialist personalised palliative care delivered by primary, community, acute and urgent care services, as well as specialists in palliative care.
A targeted response to care concerns is required based on biological rather than chronological and stereotypical responses. Whilst the NHS has set Ambitions for Palliative and End of Life Care, 2021-2026 which includes a framework of best practice developed by the National Palliative and End of Life Care Partnership, they are currently not resourced to deliver it. Having multiple care professionals delivering poorly coordinated services leads to mistakes and confusion, with poor outcomes.
There needs to be more alignment between policy and vision so that funding, regulation, workforce and performance policies match the intention of changing the focus of the health and care system towards primary and community health and care services.
The King’s Fund 7
My whole mind is set on getting decent carers, get that out of the way and I don’t think I’d have a worry in the world.
Dave, PALLUP study participant
Listening to older people: What matters to them?
University of Surrey’s, PALL UP study has been listening to the voices of older people with frailty/ MLTC living in the community, their families, and carers, to understand needs in the last phase of life, and how services and systems can change to meet them. By listening to the clients’ needs policy makers will be better placed to develop more effective services to support people with frailty/ MLTC to live the fullest lives possible in their final years. Joining up services is essential, involving the ‘right’ people, which often includes family, who in turn may require support. Building a triangle of care for the older person enables them to express their individual choices, incorporate the views of the people important to them, and service providers.

Rethinking Palliative care services
The experiences of older people with frailty/MLTC nearing the end of their lives are often poor, characterised by overtreatment in an attempt to prolong life, alongside too little palliative care. There is a fear that moving to palliative care means nothing will happen, yet the transition should be the antithesis of this.
People often fall between services focused on living independently or dying imminently and end up feeling ‘done to’ rather than ‘cared about’, with little consideration given to their desires, capabilities, and strengths.
Palliative care should support people to be as comfortable as possible while maximising the quality of their remaining life when illness is incurable. If we use need rather than expected time to death as a basis for identifying palliative care, many more would fit within current criteria for referral to specialist palliative care services.
Patients’ preferences are ultimately the key to improving overall outcomes and quality of life.
Indeed, the idea of time-based approaches – referring older people to palliative care in the last few weeks of life – is highly questionable. Instead, the focus should be on a holistic assessment of needs, met with tailored care, when someone has been identified as having complex care needs.
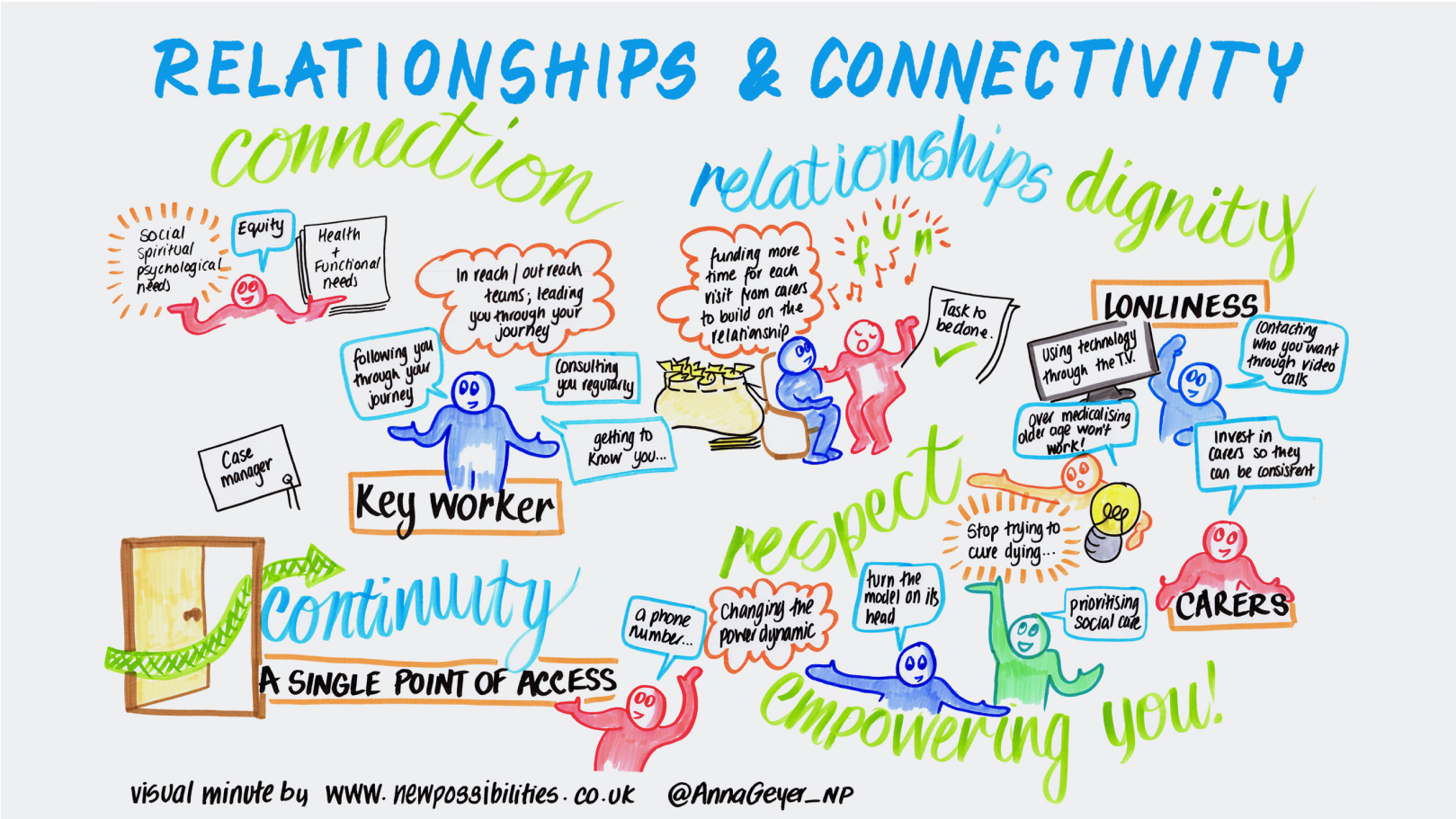
Relationships and connectivity sit at the heart of this person-centred approach to care: recognising and understanding each person’s physical, psychological, social, spiritual, and practical needs and concerns, encompassing both living and dying. Sadly, the voices of older people are often overlooked, such as in consenting to a particular service or treatment.
Older people must be seen as part of the solution, not the problem. Having choices and independence is important, and the progressive loss of independence causes frustration and fear.
Policy recommendations
- Palliative care for older people with progressive frailty/ MLTC needs to be remodelled, moved upstream, and transformed into a service for all. There is no alternative, the number of people aged 85 and over in the UK is projected to rise from an estimated 1.6 million in 2021 (2.5% of the total population) to 2.6 million by 2036 (3.5%), this upward trend will continue9.
- Different ways of working, different partnerships and a sharing of power are required to enable a focus more on a holistic assessment of needs rather than a focus on diagnosis and prognosis.
- Moving palliative care upstream requires investment in upskilling the silent workforces of paid domiciliary and unpaid family carers.
This includes training to:
- understand frailty and how to identify and assess needs.
- develop person-centred approaches to care.
- communicate effectively and compassionately.
- collaborate and integrate with other agencies and professionals.
- A single point of access for all care needs is essential. Clinical services often prioritise assessment and response to physical needs. Yet social and practical needs are often prioritised by older people.
- A public education programme is required which focuses on frailty awareness, individualised care, understanding the ageing journey and palliative care. As a society we have a civil and moral responsibility to care for the older generation, but families and friends often feel ill-equipped to support.
- Healthy Ageing must include Healthy Dying. We need to find ways to break the taboo and support honest conversations about end of life and dying to ensure life is lived to the highest quality possible.
- A Commissioner for Older People and Ageing should be established as an independent champion for older people in England. Supporting this Call to Action would facilitate long-term planning, address inequalities, and help government deal with the challenges of an ageing population.
Hospitals are the most costly way to manage health and yet they have become the first resort for many patients. There are more imaginative solutions than simply building more ‘sickness factories’.
The Times Health Commission10
About the author
Caroline Nicholson is Professor of Palliative Care and Ageing in the School of Health and Medical Sciences at the University of Surrey. Contact Professor Nicholson at c.nicholson@surrey.ac.uk if you would like to learn more about her research, invite her to speak at your event, or collaborate with the Living and Dying Well Team11
References
- Nicholson CJ, Combes S, Mold F, King H, Green R. Addressing Inequality in Palliative Care Provision for Older People Living with Multimorbidity.
- Equity in the Provision of Palliative Care in the UK: Review of Evidence.
- A Report into the State of Health and Social Care in Britain Today. The Times Health Commission, 2024.
- Report of the Lancet Commission on the Value of Death: Bringing Death Back into Life, 2022.
- Nicholson CJ, Combes S, Mold F, King H, Green R. Addressing Inequality in Palliative Care Provision for Older People Living with Multimorbidity.
- Nicholson CJ, (2023), A New Approach to Older People’s End of Life Care: Living and Dying Well, 2023.
- Baird B, Fenney, D, Jeffries, D, Brooks, A Making Care Closer to Home: Refocusing the System to Primary and Community Care, The King’s Fund, February 2024.
- CMO Annual Report, Health in An Ageing Society, 2023
- National Population Projections: 2021-based on Interim Analysis of 2021 Consensus, ONS January 2024.
- IA Report into the State of Health and Social Care in Britain Today. The Times Health Commission, 2024.
- The Living and Dying Well Team would like to acknowledge the editorial support received from Richard Vize.